
Cultivating the Myth of Transparency
New Brunswick Public Health obscured Covid-19 death metrics in the name of convenience

PoPNB recently received responses to two Right to Information (RTI) requests for records related to the change in definition of a “Covid-19 death” and what impact the change had on reported data. Information contained in the responses implies an interest in convenience at the expense of public awareness, reveals unreported historical data, and confirms fears of dramatic underreporting.
The Problem and its History
Since the onset of the Covid-19 pandemic, the Public Health Agency of Canada (PHAC) has published case definitions for Covid-19 related infections, admissions to hospital and/or intensive care, and deaths.
From the time it was first published, PHAC’s definition of a “deceased case” has remained consistent.
Deceased case
A probable or confirmed COVID-19 case whose death resulted from a clinically compatible illness, unless there is a clear alternative cause of death identified (e.g., trauma, poisoning, drug overdose).
A Medical Officer of Health, relevant public health authority, coroner or medical examiner may use their discretion when determining if a death was due to COVID-19, and their judgement will supersede the above-mentioned criteria.
A death due to COVID-19 may be attributed when COVID-19 is the cause of death or is a contributing factor.
New Brunswick Public Health adopted this case definition and reported metrics based upon it for three and a half years.
In September 2023 the Department of Health consolidated its Covid-19 and Influenza reporting into a single “Respiratory Watch” report. The new report contained most of the metrics the public had become accustomed to, however, without any clear warning that the definitions of those metrics had been revised.

As of the very first Respiratory Watch report, a Covid-19 death was redefined as
A confirmed case who was admitted to hospital and whose death occurred during their stay. A death due to COVID-19 or influenza does not mean that it was necessarily the primary or contributing factor to the cause of death.
There are three important things to note here.
First, only people admitted to hospital were now being counted as “deceased cases” and were being counted regardless of whether Covid-19 was the cause of their hospital admission. Any Covid-19 related death that occurred outside of a select number of medical buildings in the province were now omitted.
Second, confirmed Covid-19 cases who died during their hospital stay were counted as “deceased cases” regardless of whether Covid-19 was a direct or antecedent cause of their death, aligning the data with twisted and erroneous convoy denialism.
Third, nobody noticed…
There seemed to be an ubiquitous lack of comprehension regarding the definition change, and it was telegraphed repeatedly. News media continued to report on Covid-19 fatalities as though nothing had changed. In fact they still do to this day. This very week the Telegraph-Journal ran the headline “Flu, COVID kill three more New Brunswickers” despite the fact that there is no confirmation whatsoever as to whether Covid-19 or Influenza was the root cause of these deaths.

To their credit, many news outlets ran stories in October 2023 questioning the revised definition and seeking clarification from government officials who offered vague justifications and reassurances about more timely tracking. Once the stories of the changes were published, journalists could not reasonably justify dedicating limited column space to re-qualify the data coming from New Brunswick Public Health in every weekly update; nor should it be their job to do so.
This leaves anyone who missed the explanation (or did not commit it deeply enough to their memory) with little choice but to interpret headlines literally. Even those who could arguably be expected to maintain a more fulsome understanding of the Public Health data have been prone to make the same mistake.
In January, Green Party leader David Coon took to social media to lament the state of New Brunswick’s Covid-19 precautions, citing (and inadvertently misdefining) the data provided by New Brunswick Public Health.

One is hardly at fault for misinterpreting these numbers. The terminology invokes a vernacular which never suggests a need for deeper clarity. It is safe to say a reader could not be blamed for concluding “gunshot deaths” meant deaths attributable to gunshots, not people shot in hospitals.
It is a passive but thorough condemnation of Public Health’s professed transparency when numerous journalists and members of the legislative assembly can publicly infer incorrect conclusions from reported data and never be corrected.
It is important to state that we are not suggesting currently published Covid-19 metrics are exaggerated by nature of them including people who died both with and from the virus. Quite the opposite. The redefined deceased case count is absolutely undercounted due to it being limited to only those who died inside a New Brunswick hospital.
The new definition, while undercounting actual virus related mortality, also serves to underpin conspiracy theorists by giving credence to the frequently stated (and until the definition change, thoroughly baseless) denialist retort of “did they die from Covid or with Covid?” It allows space for doubt and the minimization of the very real issues with comorbidity by providing minimizers with easy fuel to dismiss Covid deaths as exaggerated or outright false.
Additionally, the change in how Covid-19 mortality is counted causes an irreconcilable rift in our historical data. All information published since September 2023 exists within its own contextual bubble, preventing us from making any material comparison to previous periods of the pandemic.
So why did this happen?
The Reasoning and the Results
Because we wanted to know why the nationally agreed upon definition was changed, on January 8, 2025 PopNB submitted a RTI request to the Department of Health for records referenced during, related to, or produced as a result of the change in definition of "deceased case" of Covid-19.
Because we wanted to directly measure the impact the redefinition had on reported metrics, on the same day PoPNB submitted a RTI request to Service New Brunswick for up-to date monthly Covid-19 deaths for 2023 as determined by the previous definition (deaths determined by the attending physician to be Covid-19 related, ie. identified that Covid-19 was a primary or antecedent contributing factor). Because of the substantial lag in provincial death reporting, we had to wait until the end of 2024 to obtain the complete record of 2023 deaths.
Both RTIs were submitted in the interest of uncovering the truth, because immediately following New Brunswick’s redefinition of Covid-19 death, then Chief Medical Officer of Health Jennifer Russell offered an anodyne but unconvincing rationale for the change in an interview with CBC. In the interview she stated that “it makes sense to monitor [influenza and Covid-19] together so that New Brunswickers can be informed of the impacts these diseases are having on the health of the population” and that “the new format reflects similar reporting approaches in other provinces, including British Columbia, Alberta, Manitoba, Ontario, and Saskatchewan.”

We have learned countless times since March 2020 that we trust Russell’s words at our peril. Neither Alberta, nor Manitoba, nor Ontario, nor Saskatchewan revised their definitions of a Covid-19 death, and while British Columbia did redefine Covid-19 death in a similar fashion to New Brunswick, it also began including additional contextual information on the percentage of deaths directly attributable to the virus.
The Public Health rhetoric surrounding changes to Covid-19 reporting has always been framed as being in service to the public interest, however when Russell stated this change “makes sense,” we would have been wrong to infer that there was “sense” provoking any effort toward amelioration. Historically, when the office of the CMOH evokes “sense” it means forthcoming changes will serve their workload, their narrative, or both.
The first response we received from the Department of Health confirms this.
In a slide deck titled “Covid-19 and Influenza: Integration Plan” dated March 17, 2023 we can see Public Health’s painfully contrived justification for discontinuing fulsome Covid reporting in New Brunswick. Immediately the goal of the integrating reporting for the two viruses is made, namely to bring all Covid-19 reporting methodologies and definitions in line with those associated with influenza, because that’s what we’ve always done.
It is difficult to not see the innate preference presented within the slide deck. Case definitions and data sources for Covid-19 all move toward the old way of doing things and there is a distinct lack of any discussion on updating influenza definitions or data to make them more unambiguous, relevant, or accurate.
Once the presentation establishes the plan’s intent to prioritize ease over efficacy, it offers as additional pretext one of the most baffling abortions of fundamental statistical concepts possibly ever committed to paper. It notes that to date (February 27, 2023) 824 Covid-19 deaths had been logged as per the current definition. The plan then juxtaposes the fact that of the 1,284 deaths which occurred within 30 days of a confirmed Covid-19 case, 800 occurred in hospital. Ignoring the fact that 460 people died within a month of Covid-19 infection without being counted, we are provided with the incomprehensibly ignorant foundation for redefining a Covid-19 death:
800 is about the same as 824, therefore all-cause deaths in Covid-19 infected hospital patients is an accurate representation of actual deaths caused by Covid-19 in the broader community.
It is difficult to overstate the depth of transgression being committed against every tenet of sensible data analysis displayed in presenting this as a reasonable conclusion. To be forced to sit with the knowledge that New Brunswick Public Health, an office which exists solely to prevent and reduce diseases and injury in our community, gleefully crippled our Covid-19 reporting due to a fundamental misunderstanding of causation versus correlation, is emotionally violent.

At the risk of creating a tangent to an already meandering conversation, we would be remiss not to mention some shocking data that was presented offhand in the slide deck with seeming detachment:
Though 824 Covid-19 deaths had been reported in New Brunswick, the number of people who died within 90 days of a Covid-19 infection was 2,987.
Though the youngest Covid-19 death was reported to be 28 years old, the youngest in-hospital death within 30 days of a Covid-19 infection was 13 years old.
These are both horrific data points that underscore Public Health’s abject failure at transparency. Presented here with indifference, this information has never been provided to New Brunswickers, likely due to it undermining the office’s long running project to normalize Covid-19 infection by equating its severity with far milder respiratory infections.
We previously requested information on 30, 60, and 90 day Covid-19 mortality and were told no data exists; a statement that we can now see was false.
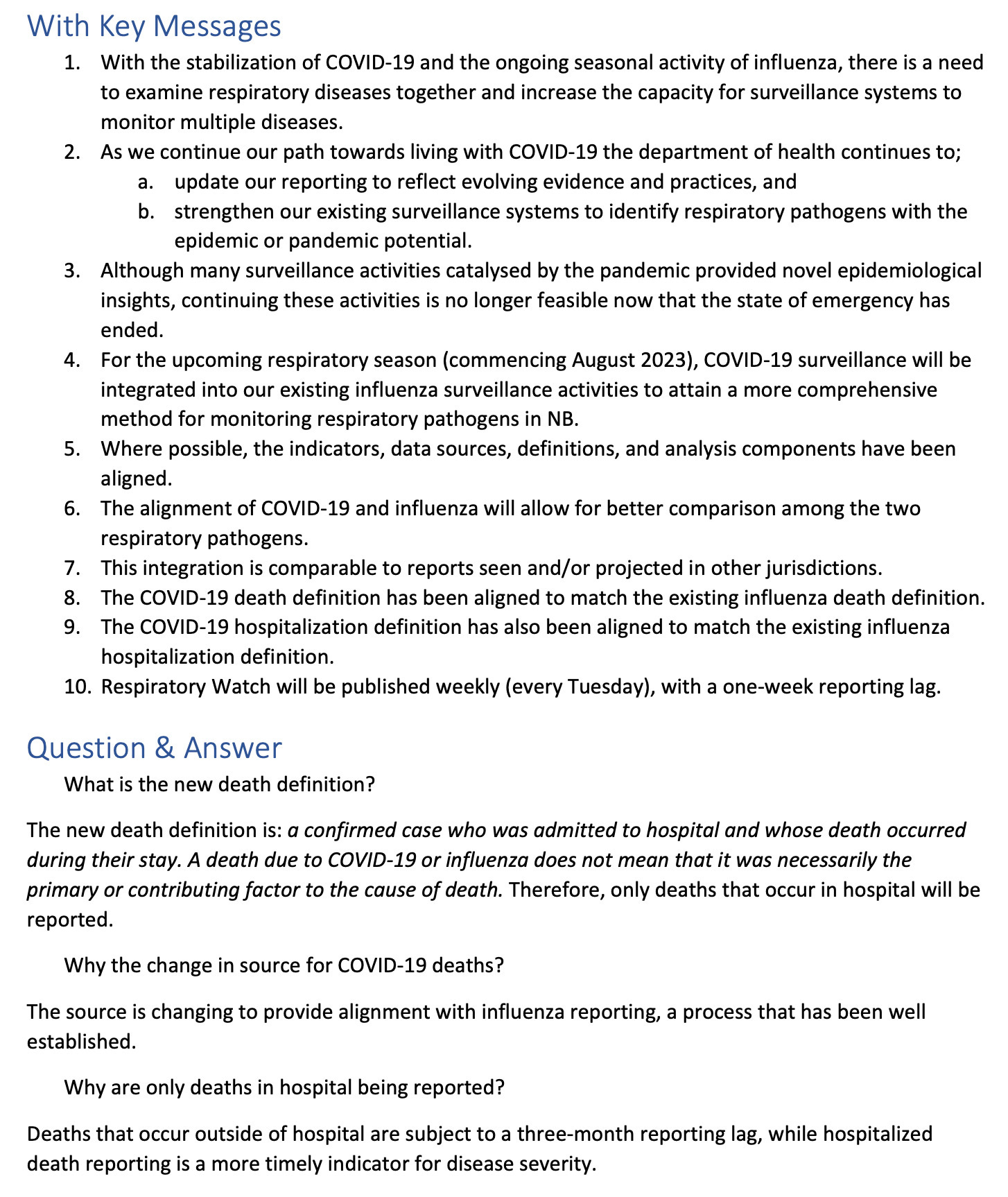
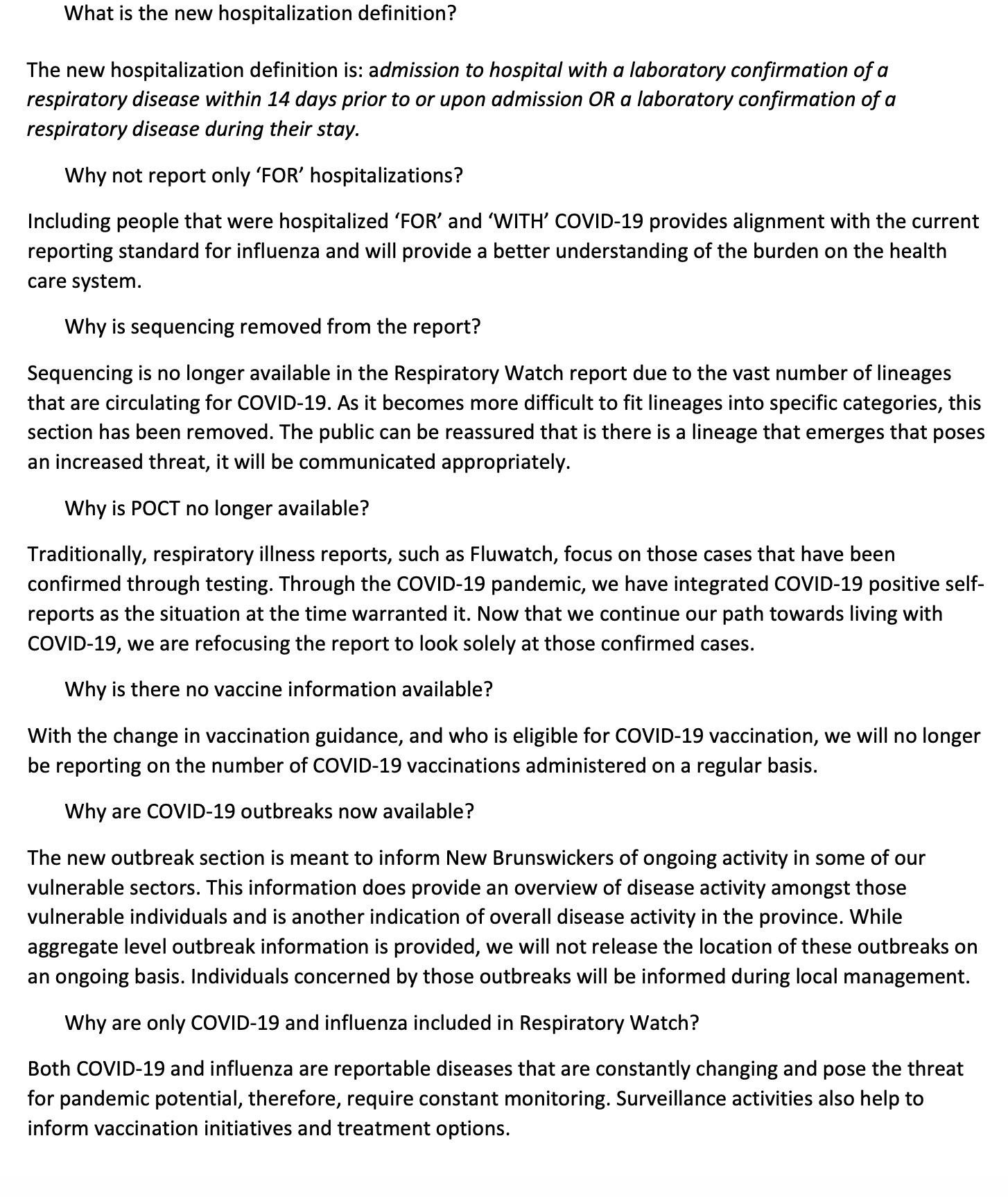
The “Covid-19 and Influenza: Integration Plan” concludes with scripted talking points and direction on how to answer the obvious questions that will be asked by anyone paying the most remote degree of attention. Permeated with buzz words and non-answers, readers are directed to provide key messages that the change will lead to “more comprehensive monitoring” and will “align” pathogens for “better comparison.” We see that the stock answer for why did you do this is given:
“The source is changing to provide alignment with influenza reporting, a process that has been well established.”
a response intended, as always, to conclude questioning rather than provide reasoning.
It should go without saying that “because that’s what we’ve always done” is never a valid consideration for any system revision, particularly one designed to provide actionable information to the public about hazards to their health.
Provided with the “rationale” for the decision to redefine Covid-19 mortality, we can pivot to the redefinition’s material impacts on metrics and reporting. Because death data from Vital Statistics lags up to a year, we were forced to wait until the end of 2024 to obtain a reasonably complete data set of 2023 deaths. We have now received that data set and can compare the number of deaths explicitly caused by Covid-19 to the number of deaths reported under both the previous definition and the redefinition.
What we can now see plainly is that
the original national definition of a Covid-19 death undercounted deaths directly and antecedently caused by Covid-19, and
the redefinition adopted by New Brunswick Public Health dramatically misleads readers and objectively obscures the severity of the ongoing pandemic.
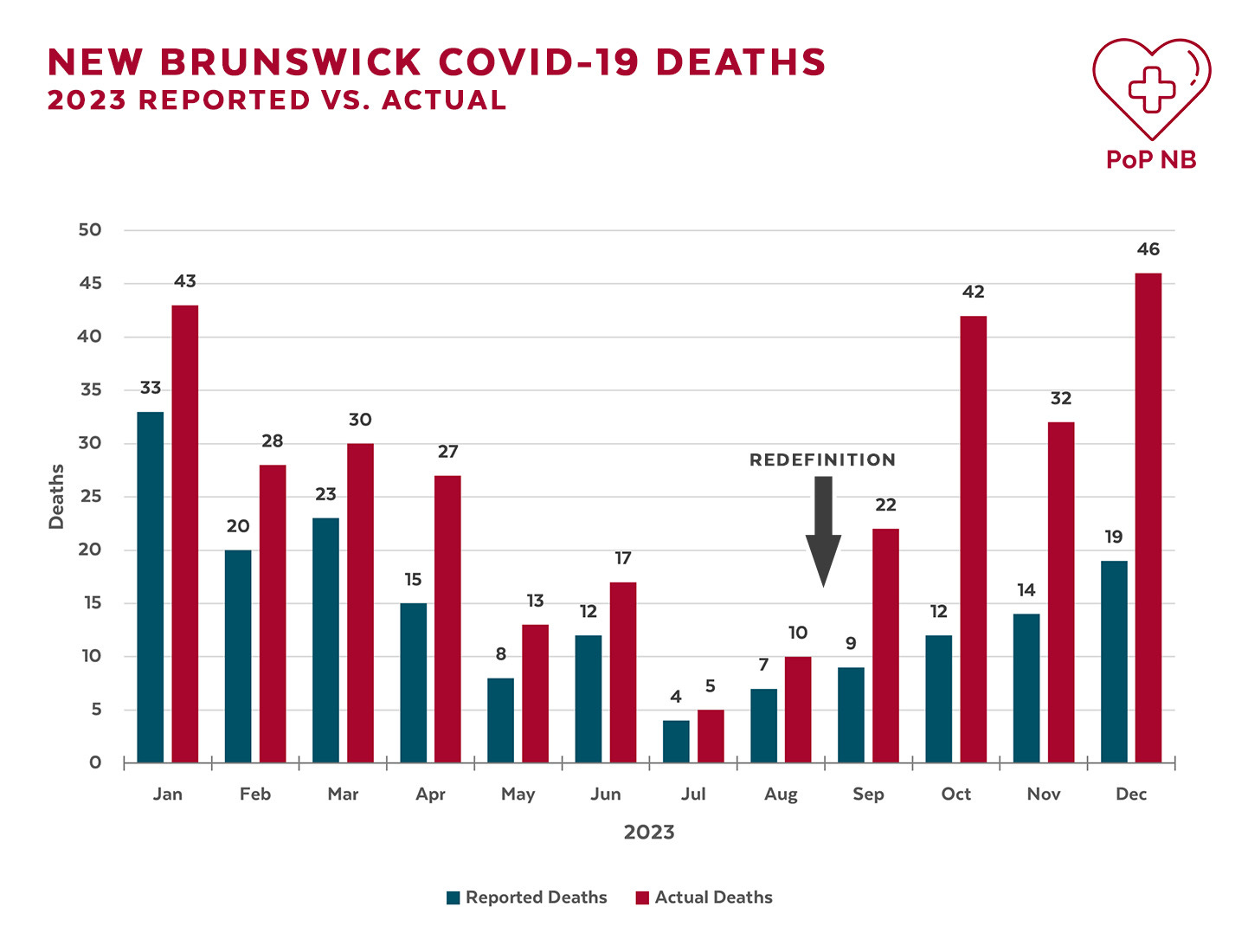
It turns out that New Brunswick Public Health’s coincidence-driven decision making made a bad situation worse, increasing the number of uncounted Covid-19 deaths from 29% to 62%. Read that again. Following Public Health’s redefinition of Covid-19 deaths, almost two of every three people who died as a result of their Covid-19 infection were not counted in reported metrics.
The continued insistence that parallels exist between Covid-19 and influenza, from reframing Covid-19 as a “respiratory illness” when it is primarily a vascular illness to lumping it in with other far less severe viruses under the umbrella of “influenza-like illnesses (ILI’s),” has diminished public awareness. It is through that diminished awareness that Public Health confidently disabled the reporting of pandemic data, further diminishing awareness.
As of March 8, 2025, Public Health has reported 1,134 Covid-19 “deaths” using their original then modified definitions. If we were to extrapolate that number based on the above information it is reasonable to conclude the actual number of New Brunswickers who have been killed by Covid-19 is between 1,700 and 4,100.
What New Brunswick Public Health is doing is the opposite of transparency. Its claims that it provides the public with the information they require to make informed decisions about their health is at best incompetent and at worst an intentional deception, and the cost of their negligence is being paid for with the literal lives of our neighbours, friends, and families.
You can read the entirety of each of the above mentioned RTI responses, as well as the responses to previous RTIs on our website.
If you would like to receive PoPNB posts in your email, please subscribe below. If you found this post helpful, please share it with your community.